




Good tidings for the people of Umerkot

Sindh province in Pakistan is widely known for its vibrant craftsmanship and rich cultural heritage. The region paints a serene picture of its desert landscapes and a myriad of colors seeping through the fabric of local clothes. However, beneath this cultural splendour, many communities grapple with the challenges of inadequate infrastructure and severe climatic conditions. They are at the mercy of recurring droughts, limited sanitation, and an escalating hunger crisis. With annual rainfall often falling below 200 mm, livelihoods are precarious, and poverty is widespread.
District Umerkot is particularly hard-hit, with many residents living below the poverty line. In this struggle for survival, basic needs often take precedence over education and healthcare. Families are forced to prioritise food and water, leaving schooling and medical care as distant concerns. Accessing private medical services is often a luxury, or, in desperate situations, a burden of debt.


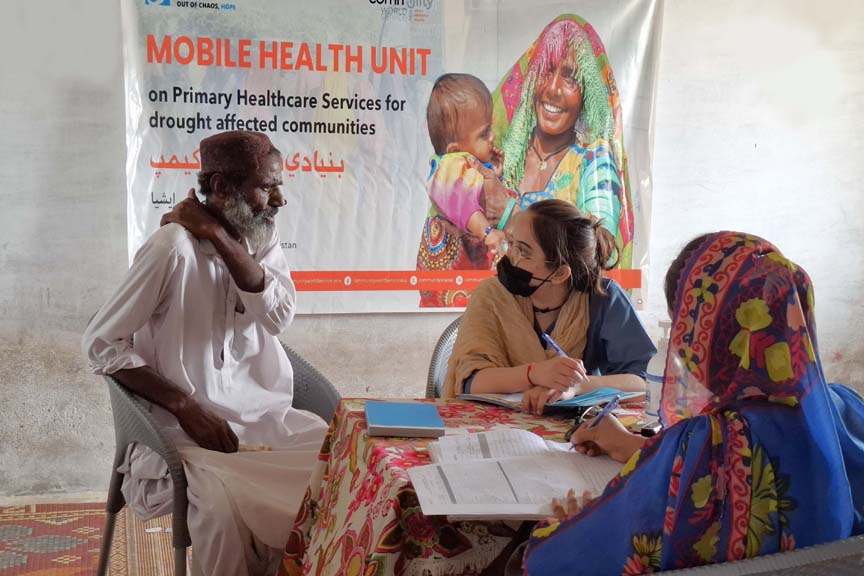









In a region where the choice between health and livelihood is a daily struggle, Community World Service Asia (CWSA) has stepped in to provide a transformative solution: a mobile health unit that delivers accessible medical assistance without requiring any sacrifice. For those who have endured years of pain and suffering from untreated illnesses, the introduction of free medical services right in their communities has been nothing short of a miracle. Previously, many had to travel long distances or sell livestock to afford treatment. Now, help is just a doorstep away.
Umerkot has a total of 42 union councils, and three of these, UC Faqeer Abdullah, Seekhro, and Kaplor, come into CWSA’s focus area. There are 153 villages in these union councils, with a combined population of nearly 85,000 people.
The medical camps are open to all; men, women, and children, but it is the women who have voiced the greatest joy and relief. As active caregivers at home and hardworking labourers in the fields, they often bear the weight of exhaustion from long hours of strenuous work, limited rest, and neglecting their own well-being. This relentless strain leaves them with weakened immune systems, making them more susceptible to illness. Common health issues include leg pain, scabies, digestive disorders, and complications related to pregnancy, both antenatal and postnatal, all exacerbated by the lack of clean water and proper sanitation.
In UC Kaplor, there are no hospitals or clinics nearby. The only option is to travel 50 km to Umerkot city, a journey that takes hours on foot under the scorching sun, often with only a small bottle of water for sustenance.
Radha, a mother of five from Kaplor, shared her experience of accessing medical services. “Previously, even for a minor illness, we had to travel all the way to Umerkot city for a check‑up. This journey was not only exhausting but also very costly. The bus fare alone was difficult to manage, not to mention the doctor’s fee and medicine bills.” To add to the hardship, women were not allowed to travel on their own, making it mandatory to be accompanied by a male guardian, doubling the expense.
She recalled how the rickety, overcrowded minivan worn thin by years of use, rattling along broken roads as one of the few lifelines connecting isolated communities to their destination. Those dust, bad air filled journeys had mothers clutching their sick children close to them, to leave them feeling even worse. The entire trip cost nearly PKR 5,000 to 10,000 (USD 17 -35), an amount that could otherwise feed their entire household. For her and countless others, the ‘free’ medical camp meant not only immediate relief but also peace of mind and dignity. Her daughter, who suffered from urinary problems, received free consultation too, reinforcing how important such interventions are when entire families and whole villages carry multiple untreated health issues.
Another recipient of the health camp, Akla, recounted the death of a relative due to the absence of an emergency health facility and lack of reliable transport. She also spoke of her daughter‑in‑law’s emergency C‑section at a city hospital, an ordeal that left the family with a bill of PKR 75,000 (USD 250). “It’s either your property or your livestock,” she said. In their case, it was livestock that had to be sold to pay the bill.
Now, apart from the mobile health units making stops from village to village, the same people battered by sickness, fatigue and torment are able to access what was once a non functional government dispensary revived again in 2025 by CWSA. The distance is cut down to merely 2km and expense to nearly none.
Both the mobile health units and the medical dispensary are staffed by a dedicated team, including a Women Medical Officer (WMO), a Lady Health Visitor (LHV), a Medical Technician, and a Community Mobiliser. This diverse team ensures efficient operations while maintaining cultural sensitivity. The WMO and LHV are responsible for examining and diagnosing patients, while the Medical Technician dispenses prescribed medications. Community Mobilisers conduct health awareness sessions that focus on disease prevention and basic health practices, including family planning counseling. These camps provide primary healthcare services and essential medicines at no cost to the community. Serious cases are referred to the nearest taluka and district hospitals for further diagnosis and treatment.
The doctors and field mobilisers prioritise solutions that are adaptable to the community’s environment and daily routines. They promote safe practices such as boiling water before drinking, frequently washing hands, thoroughly rinsing food, and using simple home remedies alongside prescribed medications.
In recognition of its supportive role, CWSA collaborates closely with the District Health Administration and other relevant stakeholders. Since launching the first camp in July 2025, the initiative has reached 56 remote villages and engaged over 26,000 participants through various project activities. To date, 150 mobile health camps have been conducted across 60 villages, providing curative health services to 17,295 individuals, along with free essential medicines and health consultations.
Additionally, the project team has held 260 health education sessions with 7,712 community members. These sessions have addressed critical topics such as maternal, newborn, and child health (MNCH), child-spacing, hygiene practices, and the prevention of common diseases. Critical cases, including malnourished children, are identified, screened, and referred to specialised healthcare facilities for advanced treatment.
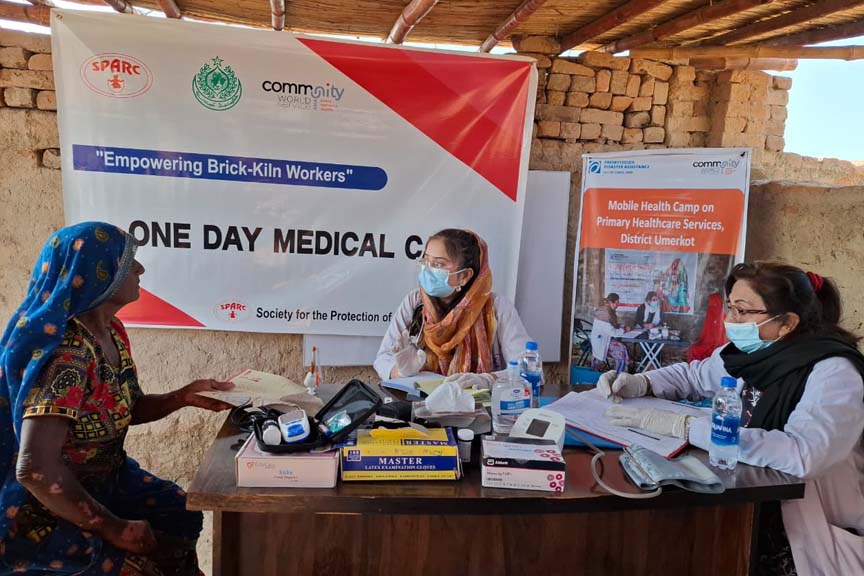
The mobile health units continue to support communities with their health and medical needs. In January of 2026, their latest stop served the brick kiln workers and their families. In collaboration with District Administration and SPARC (Society for the Protection of the Right of the Child), the initiative aimed at providing consultations, treatment, free medicines, and health awareness sessions for a segment of society very much ignored by the system, often working and living in extremely unsafe and unsuitable conditions. They remain invisible to labour protections, denied basic rights leaving them trapped in exploitative conditions with little support from formal systems. During labour, they are exposed to toxic smoke, dust, and fumes from burning wood and coal. This leads to high rates of chronic respiratory illness and other health problems.
Many workers and their families live on or near kiln sites with no access to basic amenities such as clean water, sanitation, or protective equipment, and long working hours under extreme heat only compound these risks. They are often trapped in a cycle of poverty and debt, borrowing from the kiln owners to cover basic needs, including medical expenses, with little chance of ever repaying these loans. In such conditions, health and wellbeing become secondary to survival. During this camp, 256 patients working on brick kiln sites were examined, treated, and provided essential medicine along with prevention awareness.
One worker shared his experience about the long working hours and difficult conditions faced by families at the brick kiln.
“We work here at brick kiln sites for about 12 hours a day, and sometimes even longer,” he said, adding that “most of us belong to poor families and work here together with our entire family members.”
He explained that living conditions at the site are extremely limited. “We do not have proper shelters, sanitation, or health facilities,” he said. He added that survival depends on constant labour, “For our livelihood and daily meals, we have to work very hard.”
Because of these hardships, healthcare becomes difficult to afford. “In such conditions, we cannot afford the additional burden of medical expenses,” they explained, noting that “if my family and I visit a doctor, we have to pay more than PKR 2,000 (7 USD).”
The brick kiln workers expressed appreciation for the medical support they received at the camp. These camps have not only treated thousands of patients but also restored dignity, hope, and resilience to families who had resigned themselves to suffering. The mobile health initiative has demonstrated that when healthcare is brought closer to the people, barriers of distance, cost, and neglect can be broken down, and preventable illness no longer needs to become a lifelong burden. As these units continue their journey from village to village, they stand as a testament to what is possible when communities are prioritised, partnerships are strengthened, and the health needs of even the most remote populations are met with compassion, commitment, and sustained action.

